Table of Contents
- The Two Major Divisions of the Nervous System
- Brain Anatomy
- Spinal Cord Anatomy
- Cranial and Peripheral Nerves
- How Nervous System Anatomy Connects to CPT Code Selection
- How Nervous System Anatomy Connects to ICD-10-CM
- Common Neurological Conditions and Coding Context
- Diagnostic Studies Referencing Neurological Anatomy
- How the CPC Exam Tests Nervous System Anatomy
- Common Mistakes
- Frequently Asked Questions
The nervous system coordinates and controls nearly every function in the body, and its anatomy is among the most structurally complex of any body system a coder will encounter. Neurological documentation is dense with specialized terminology — spinal levels, nerve root names, brain regions, and the distinction between central and peripheral structures — and misreading any of it can send a coder to the wrong CPT code range or the wrong ICD-10-CM chapter entirely.
This guide builds the anatomical foundation needed to interpret neurological documentation accurately: the major divisions of the nervous system, brain and spinal cord structure, the cranial and spinal nerves, and how this anatomy maps to CPT and ICD-10-CM code selection. For the surgical code range built on this anatomy, see Surgery Coding for Beginners, and for etiology/manifestation sequencing that frequently applies to neurological conditions, see ICD-10-CM Sequencing Rules.
The Two Major Divisions of the Nervous System
The nervous system is divided into two primary structural divisions.
| Division | Components | Function |
|---|---|---|
| Central Nervous System (CNS) | Brain and spinal cord | Processing and integration center; controls thought, movement, and coordination |
| Peripheral Nervous System (PNS) | Cranial nerves, spinal nerves, and all nerves outside the CNS | Carries signals between the CNS and the rest of the body |
The peripheral nervous system is further divided functionally into the somatic nervous system, which controls voluntary movement and processes conscious sensory information, and the autonomic nervous system, which controls involuntary functions like heart rate, digestion, and respiratory rate. The autonomic nervous system has two further branches: the sympathetic division (“fight or flight” response) and the parasympathetic division (“rest and digest” response), which generally act in opposition to maintain homeostasis.
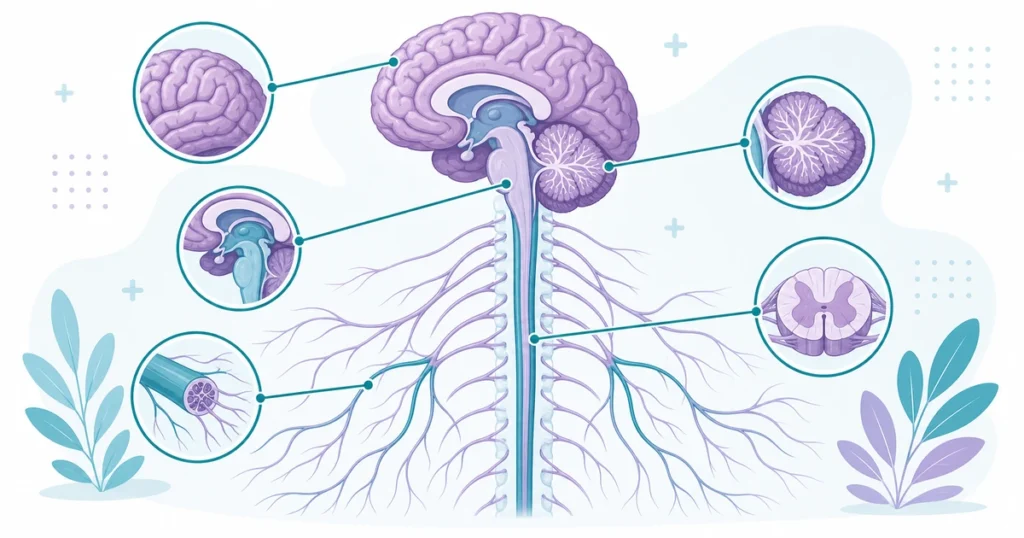
Brain Anatomy
The brain is divided into major regions, each responsible for distinct functions, and CPT and ICD-10-CM documentation frequently references these regions by name.
| Brain Region | Primary Functions |
|---|---|
| Cerebrum (frontal, parietal, temporal, occipital lobes) | Higher-order thinking, voluntary movement, sensory processing, speech, vision, memory |
| Cerebellum | Balance, coordination, fine motor control |
| Brainstem (midbrain, pons, medulla oblongata) | Vital functions — breathing, heart rate, consciousness; relay point between brain and spinal cord |
| Diencephalon (thalamus, hypothalamus) | Sensory relay (thalamus), hormone regulation and homeostasis (hypothalamus) |
The Cerebral Lobes
Each cerebral hemisphere is divided into four lobes. The frontal lobe governs voluntary movement, personality, judgment, and expressive speech (Broca’s area). The parietal lobe processes sensory information such as touch, temperature, and spatial awareness. The temporal lobe processes auditory information, memory formation, and receptive speech (Wernicke’s area). The occipital lobe processes visual information. Documentation describing the location of a stroke, tumor, or traumatic injury frequently references these lobes, and the specific lobe involved often correlates directly with the clinical symptoms described (for example, a frontal lobe injury causing personality changes, or an occipital lobe injury causing visual deficits).
Protective Structures
The brain and spinal cord are protected by three layers of connective tissue called the meninges: the dura mater (outermost, toughest layer), the arachnoid mater (middle, weblike layer), and the pia mater (innermost layer, directly adhering to neural tissue). The space between the arachnoid and pia mater, called the subarachnoid space, contains cerebrospinal fluid (CSF), which cushions the brain and spinal cord. Meningeal terminology is directly relevant to coding — conditions such as epidural hematoma (above the dura), subdural hematoma (below the dura, above the arachnoid), and subarachnoid hemorrhage (within the subarachnoid space) are distinguished entirely by which meningeal layer the bleeding occurs relative to, and each has distinct ICD-10-CM codes.
Spinal Cord Anatomy
The spinal cord runs from the base of the brain through the vertebral canal and is organized into segments that correspond to the vertebral levels of the spine.
| Spinal Region | Number of Segments | Common Abbreviation |
|---|---|---|
| Cervical | 8 (C1–C8) | C-spine |
| Thoracic | 12 (T1–T12) | T-spine |
| Lumbar | 5 (L1–L5) | L-spine |
| Sacral | 5 (S1–S5, fused) | Sacrum |
| Coccygeal | 1 (fused) | Coccyx |
Spinal nerve roots exit the vertebral column at each corresponding level, and documentation of radiculopathy (nerve root compression) or spinal surgery specifies the exact level involved (for example, “L4-L5 disc herniation with L5 radiculopathy”). Precise level identification is required for both CPT spinal procedure codes, which are level-specific, and ICD-10-CM codes describing the affected spinal region.
Cranial and Peripheral Nerves
Twelve pairs of cranial nerves emerge directly from the brain and brainstem, each controlling specific sensory or motor functions of the head and neck (with one exception — the vagus nerve, which extends into the thorax and abdomen). Common cranial nerves referenced in clinical documentation include the optic nerve (CN II, vision), the trigeminal nerve (CN V, facial sensation and chewing), the facial nerve (CN VII, facial movement), and the vagus nerve (CN X, parasympathetic control of heart, lungs, and digestive tract).
Spinal nerves branch from the spinal cord at each vertebral level and eventually form the major peripheral nerves of the limbs and trunk through networks called plexuses — the brachial plexus (upper limb, formed from C5–T1 nerve roots) and the lumbosacral plexus (lower limb, formed from L1–S4 nerve roots) being the two most clinically significant. Peripheral nerve injuries and repairs, such as carpal tunnel release affecting the median nerve, are coded based on the specific named nerve involved.
How Nervous System Anatomy Connects to CPT Code Selection
The Nervous System subsection of CPT (61000–64999) is organized by anatomical region — skull, meninges, brain, spinal cord, spine, and peripheral nerves — and by procedure type within each region (injection, incision, excision, repair, neurostimulator procedures). Accurately identifying whether a procedure involves the central nervous system (brain, spinal cord) versus the peripheral nervous system (spinal or peripheral nerves) is the first branch point in selecting the correct code family, since these are organized in largely separate parts of the subsection.
Spinal procedures additionally require identifying the specific vertebral level(s) involved and the approach (anterior, posterior, or combined), both of which materially change CPT code selection — a fact that connects directly back to the directional and positional terminology covered in general anatomy.
How Nervous System Anatomy Connects to ICD-10-CM
Diseases of the nervous system are classified primarily in ICD-10-CM Chapter 6 (G00–G99), covering conditions such as epilepsy, migraine, Parkinson’s disease, multiple sclerosis, and peripheral neuropathies. However, neurological manifestations of conditions classified elsewhere — such as diabetic neuropathy or dementia in Parkinson’s disease — are coded using etiology/manifestation pairs, where the underlying disease is sequenced first and the neurological manifestation second.
Traumatic brain and spinal cord injuries are coded from Chapter 19 (Injury, poisoning, S00–T88), and these codes require the 7th character extension to indicate encounter type, along with, for many traumatic brain injury codes, an indication of loss of consciousness duration when documented.
Common Neurological Conditions and Coding Context
| Condition | System Affected | ICD-10-CM Category |
|---|---|---|
| Epilepsy | CNS (brain, abnormal electrical activity) | G40.- |
| Migraine | CNS (vascular/neurological) | G43.- |
| Parkinson’s disease | CNS (basal ganglia) | G20 |
| Multiple sclerosis | CNS (demyelinating) | G35 |
| Peripheral neuropathy | PNS | G60–G65 (or diabetes combination code if diabetic) |
| Carpal tunnel syndrome | PNS (median nerve) | G56.0- |
Stroke Terminology
Stroke (cerebrovascular accident) coding depends heavily on distinguishing the underlying mechanism, since this drives both the code category and the clinical severity implied. An ischemic stroke results from a blocked blood vessel cutting off blood supply to part of the brain, coded from category I63. A hemorrhagic stroke results from bleeding into or around brain tissue, coded from categories I60–I62 depending on the specific location (subarachnoid, intracerebral, or other nontraumatic hemorrhage). A transient ischemic attack (TIA) produces stroke-like symptoms that fully resolve, typically within 24 hours, and is coded separately from a completed stroke using category G45. Because these three conditions use entirely different code categories despite overlapping symptoms, correctly identifying the documented mechanism is essential.
Diagnostic Studies Referencing Neurological Anatomy
Several diagnostic procedures generate reports that lean heavily on the anatomical terminology covered above. Electroencephalography (EEG) records electrical activity across regions of the cerebral cortex and is used to evaluate seizure activity. Electromyography (EMG) and nerve conduction studies (NCS) evaluate peripheral nerve and muscle function, often ordered together to localize the site of a peripheral nerve injury such as carpal tunnel syndrome or radiculopathy. Lumbar puncture (spinal tap) collects cerebrospinal fluid from the subarachnoid space at the lumbar level, below the point where the spinal cord itself ends, to avoid injuring neural tissue. Recognizing which anatomical structure each study evaluates helps a coder connect the diagnostic procedure code to the correct corresponding diagnosis code on the same claim.
How the CPC Exam Tests Nervous System Anatomy
Pattern 1 — CNS vs PNS Identification
The scenario describes a procedure or condition and asks whether it involves the central or peripheral nervous system, which determines which part of the CPT Nervous System subsection or which portion of ICD-10-CM Chapter 6 applies.
Pattern 2 — Meningeal Layer and Hemorrhage Type
The question describes a head injury with bleeding at a specific location relative to the meninges (epidural, subdural, subarachnoid) and asks for the correct diagnosis code. You must know the anatomical relationship between the meningeal layers to correctly classify the hemorrhage type.
Pattern 3 — Spinal Level Specificity
The scenario provides an operative report referencing a specific spinal level (for example, “L4-L5”) and includes answer choices for adjacent but different levels. The correct answer requires precisely matching the documented level.
Pattern 4 — Etiology/Manifestation for Neurological Complications
The scenario describes a systemic disease (diabetes, Parkinson’s disease) with a neurological manifestation (neuropathy, dementia), and the correct answer sequences the underlying disease first and the neurological manifestation second, per etiology/manifestation coding rules.
Common Mistakes
Confusing CNS and PNS structures. The brain and spinal cord are CNS; all nerves branching from them, including cranial and spinal nerves, are PNS. This distinction determines which CPT code family and which portion of the ICD-10-CM nervous system chapter applies.
Misidentifying meningeal hemorrhage location. Epidural, subdural, and subarachnoid hemorrhages are distinguished entirely by their location relative to the dura, arachnoid, and pia mater. Confusing these layers leads to selecting the wrong diagnosis code.
Missing spinal level specificity. Spinal procedure and diagnosis codes are frequently level-specific. Reporting a general “spine” code when the documentation specifies an exact vertebral level under-codes the encounter’s specificity.
Reversing etiology/manifestation order for neurological complications. When a systemic disease causes a neurological complication, the underlying disease is always sequenced first and the neurological manifestation second — reversing this order is a mandatory sequencing error.
Assuming all twelve cranial nerves stay within the head and neck. The vagus nerve (CN X) is a notable exception, extending into the thorax and abdomen to provide parasympathetic control of the heart, lungs, and digestive organs. Documentation involving vagus nerve procedures or dysfunction may describe symptoms outside the head and neck region.
5 quick questions drawn from this guide. Click an answer to check it — explanations appear as you go.
1. The central nervous system (CNS) consists of the:
2. How many pairs of cranial nerves are there?
3. The largest part of the brain, responsible for higher functions, is the:
4. The autonomic nervous system controls:
5. A “CVA” documented in a chart most often refers to a:
Frequently Asked Questions
What is the difference between the central and peripheral nervous system?
The central nervous system (CNS) consists of the brain and spinal cord, serving as the body’s processing and integration center. The peripheral nervous system (PNS) consists of all the cranial and spinal nerves that carry signals between the CNS and the rest of the body. This distinction determines which CPT code family and which section of ICD-10-CM Chapter 6 applies to a given condition or procedure.
What are the three layers of the meninges?
The meninges consist of the dura mater (outermost, toughest layer), the arachnoid mater (middle, weblike layer), and the pia mater (innermost layer, directly covering brain and spinal cord tissue). The exact location of a hemorrhage relative to these layers — epidural, subdural, or subarachnoid — determines which diagnosis code applies.
Why does spinal level matter for coding?
Both CPT spinal procedure codes and ICD-10-CM diagnosis codes are frequently specific to the exact vertebral level involved, such as L4-L5. Reporting a general spine code without the documented level, or reporting the wrong level, results in an inaccurate or incorrect code even if the general procedure or condition type is correct.
How are neurological complications of systemic diseases coded?
Neurological complications of systemic diseases, such as diabetic neuropathy or dementia in Parkinson’s disease, typically use etiology/manifestation coding. The underlying systemic disease is sequenced first as the etiology, and the neurological condition is sequenced second as the manifestation. This order is mandatory and cannot be reversed.
How many cranial nerves are there?
There are twelve pairs of cranial nerves, each controlling specific sensory or motor functions primarily in the head and neck. The vagus nerve (CN X) is a notable exception, extending beyond the head and neck to provide parasympathetic control over the heart, lungs, and digestive organs.