CPT add-on codes are one of the first special code types that beginner coders encounter in the CPT codebook. They look like regular CPT codes but come with a very important rule: they can never be reported alone. Understanding CPT add-on codes — how to identify them, when to use them, and what rules apply — is tested on the CPC exam and comes up regularly in real-world coding.
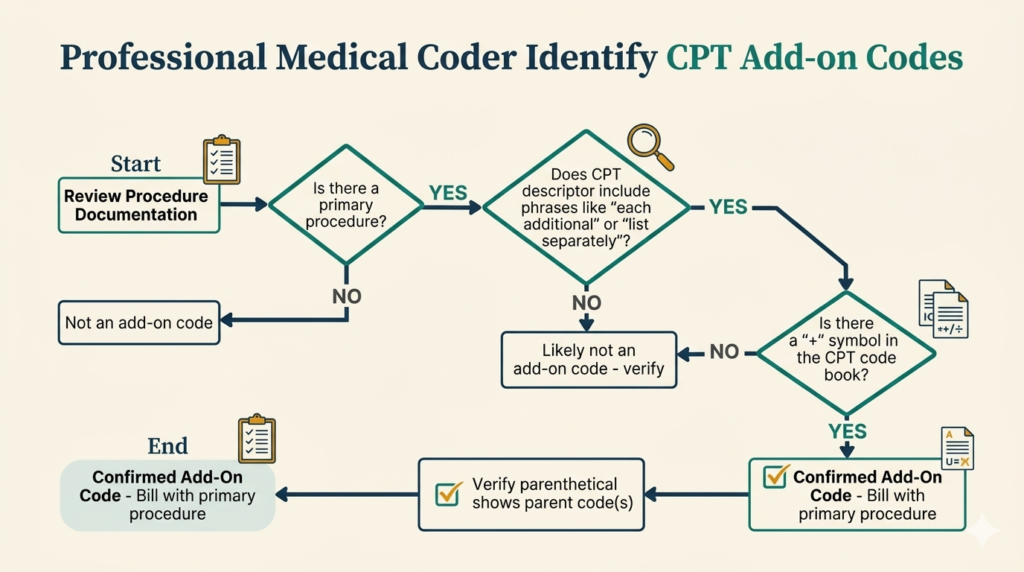
An add-on code is a CPT code that describes a service that is always performed in addition to a primary procedure — never by itself. CPT Add-on codes are marked with a plus sign (+) in the CPT codebook, making them easy to identify visually. They represent additional work, additional units of service, or additional complexity that goes beyond the primary procedure.
CPT Add-on codes were created because some procedures are commonly performed in multiples or have optional additional components that not every patient receives. Instead of creating entirely separate codes for every variation, the AMA uses CPT add-on codes to capture the additional service efficiently.
There are three ways to identify add-on codes in the CPT codebook:
| Add-On Code | Description | Primary Code(s) |
|---|---|---|
| +11001 | Debridement of additional 20 sq cm or part thereof (each additional) | 11000 |
| +11008 | Removal of prosthetic material or mesh, abdominal wall for infection (list separately) | 10004–49999 |
| +15301 | Autograft, skin — each additional 100 sq cm | 15300 |
| +99292 | Critical care, each additional 30 minutes | 99291 |
| +99354 | Prolonged service, each additional 30 minutes (outpatient) | E&M codes |
| +01953 | Anesthesia for burn excision/debridement, each additional 9% of body surface | 01952 |
This is the fundamental rule. An add-on code without its primary procedure code on the same claim will be denied by the payer. Always ensure the primary code is listed first on the claim.
Modifier -51 is used when multiple procedures are performed at the same session — it signals that a procedure is secondary and should be reimbursed at a reduced rate. Add-on codes are automatically exempt from modifier -51 because they are already priced to reflect their supplemental nature. Never append modifier -51 to an add-on code.
Do not confuse CPT add-on codes with modifier-51-exempt codes. Modifier-51-exempt codes (marked with ⊘ in the CPT book) are not CPT add-on codes — they are standalone codes that simply do not receive the multiple procedure reduction. Add-on codes are a separate, distinct category.
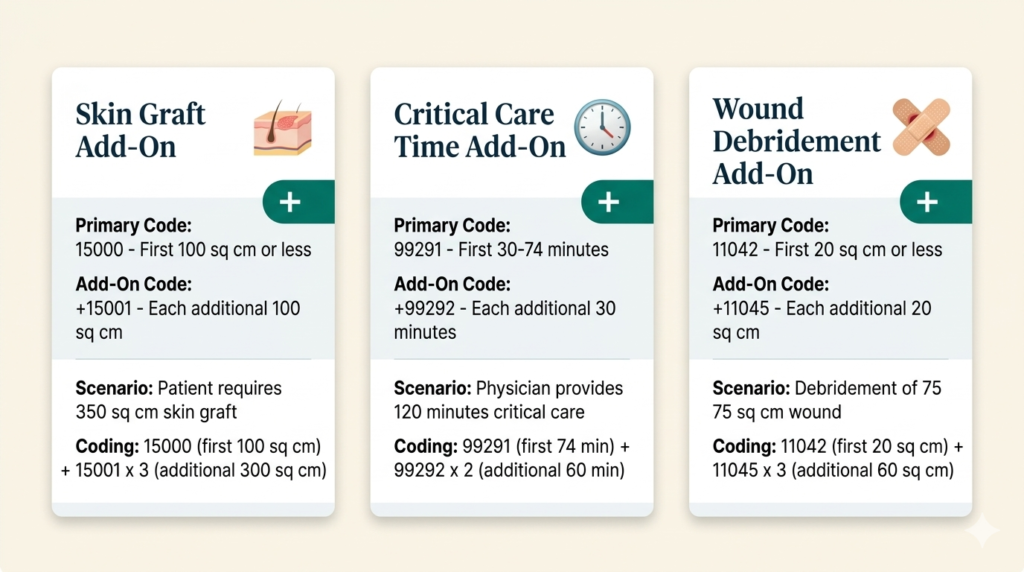
Some add-on codes are reported multiple times on the same claim to represent the number of additional increments performed. For example, if a critical care patient required 99291 (first 30–74 minutes) plus three additional 30-minute periods, you would report 99292 three times (or with 3 units).
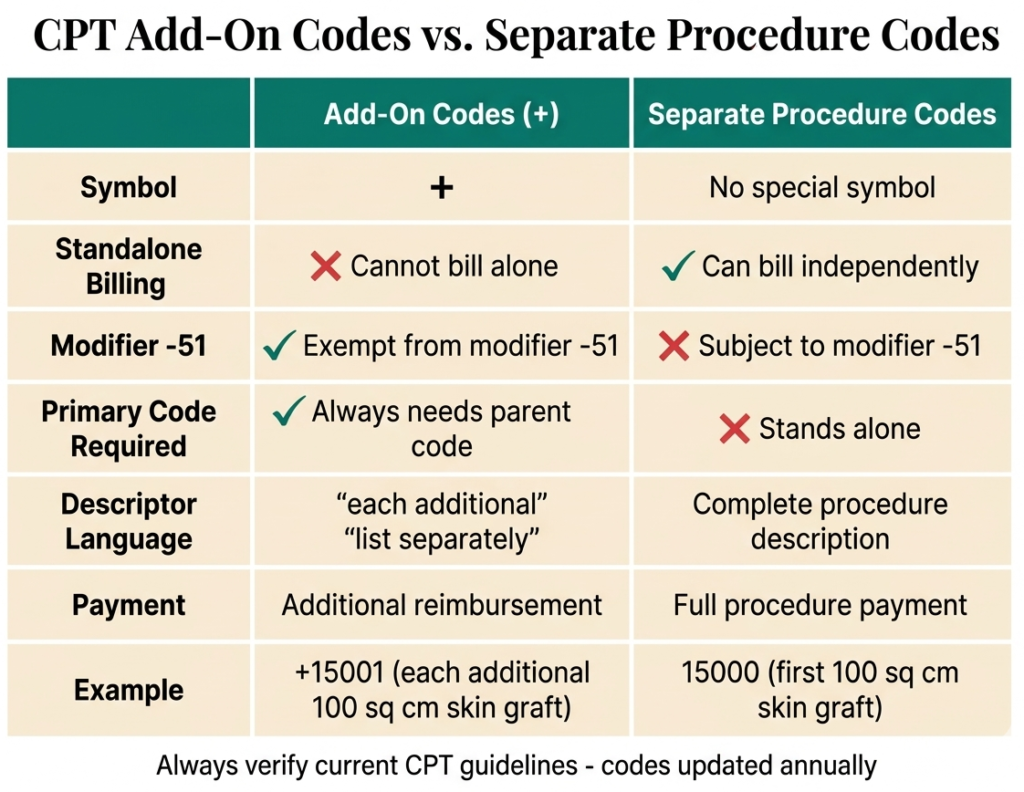
Add-on codes are sometimes confused with codes marked “separate procedure” in the AMA CPT codebook. These are completely different concepts:
Anesthesia coding is unique in the CPT codebook — it uses a completely different payment system from other sections. Instead of a flat fee per procedure, anesthesia is calculated using a unit-based formula that accounts for the complexity of the procedure, the time involved, and the patient’s medical condition. This guide explains the entire system from scratch so you can confidently tackle anesthesia questions on the CPC exam.
When a surgeon performs a procedure, you select one CPT code that describes what was done and the payer reimburses a set fee. Anesthesia works differently. The anesthesiologist or CRNA is paid based on a formula that combines three types of units multiplied by a conversion factor — a dollar amount per unit set by each payer.
The anesthesia CPT codes (00100–01999) are organized by the body area or type of procedure for which anesthesia is administered — not by what the anesthesiologist specifically does. One anesthesia code covers the entire anesthetic management of a case.
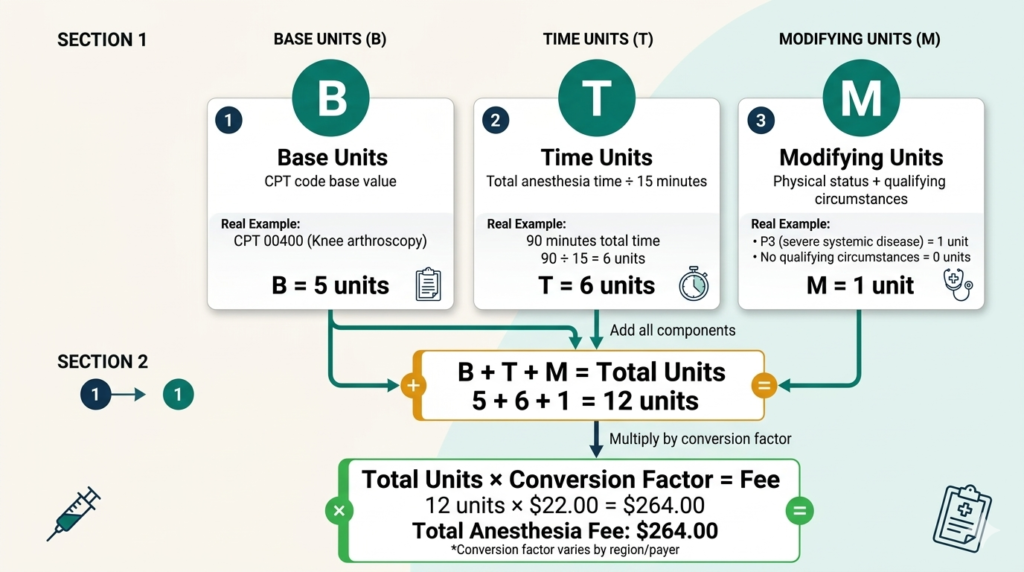
The anesthesia coding BTM formula calculates fees as follows:
B = Base Units · T = Time Units · M = Modifying Units
Each anesthesia CPT code is assigned a specific number of base units by the American Society of Anesthesiologists (ASA). Base units reflect the complexity and risk of providing anesthesia for a particular type of procedure. Simple procedures have fewer base units; complex, high-risk procedures have more. For example anesthesia for a routine knee arthroscopy might have 3 base units while anesthesia for open heart surgery might have 20 or more.
Time units are calculated based on how long the anesthesia service lasted. The standard calculation is one time unit for every 15 minutes of anesthesia time. Anesthesia time begins when the anesthesiologist starts preparing the patient for induction and ends when the anesthesiologist is no longer in personal attendance — typically when the patient is safely transferred to post-anesthesia care.
Modifying units are added based on special circumstances that increase the complexity or risk of the anesthetic. The two main sources of modifying units are physical status modifiers and qualifying circumstances.
Physical status modifiers describe the patient’s overall health and pre-existing medical conditions at the time of surgery. They are appended to the anesthesia CPT code and add modifying units to the anesthesia calculation. They are designated P1 through P6:
| Modifier | Description | Units Added | Example |
|---|---|---|---|
| P1 | Normal healthy patient | 0 | Healthy 25-year-old for elective surgery |
| P2 | Patient with mild systemic disease | 0 | Well-controlled type 2 diabetes, mild hypertension |
| P3 | Patient with severe systemic disease | 1 | Poorly controlled diabetes, COPD, morbid obesity |
| P4 | Patient with severe systemic disease that is a constant threat to life | 2 | Recent MI, severe cardiac dysfunction, sepsis |
| P5 | Moribund patient not expected to survive without the operation | 3 | Ruptured aortic aneurysm, massive trauma |
| P6 | Brain-dead patient — organ donor | 0 | Organ procurement surgery |
Qualifying circumstances are special conditions that significantly affect the character of the anesthesia service provided. They are reported using add-on codes from the Medicine section of CPT (99100–99140) and add additional modifying units:
| Code | Circumstance | Units Added |
|---|---|---|
| 99100 | Anesthesia for patient of extreme age — younger than 1 year or older than 70 | 1 |
| 99116 | Utilization of total body hypothermia | 5 |
| 99135 | Controlled hypotension | 5 |
| 99140 | Emergency conditions — delay in treatment would lead to significant increase in threat to life | 2 |
A 72-year-old patient with poorly controlled COPD (P3) undergoes a total hip replacement as an emergency procedure. Anesthesia time is 2 hours (120 minutes). The anesthesia code has 10 base units. The conversion factor is $80 per unit.
When a Certified Registered Nurse Anesthetist (CRNA) provides anesthesia services, specific HCPCS modifiers are required to identify the level of physician involvement:
Bundled codes are one of the most important compliance concepts in medical coding. When two procedures are bundled together, it means one code already includes the work described by another — and billing them separately is considered improper. The National Correct Coding Initiative (NCCI) is the system that enforces these bundled code rules for Medicare and most other payers. Understanding NCCI edits and bundled codes is essential for the CPC exam and for preventing billing errors in real-world coding.
When a CPT code is said to be bundled into another, it means the work, supplies, and effort described by the smaller code are considered already included in the payment for the larger code. Billing both codes separately would result in double payment for the same service — which is a compliance violation.
Think of it like ordering a combo meal at a restaurant. If you order a burger combo that includes fries and a drink, you cannot also charge separately for the fries and the drink. The fries are bundled into the combo. Medical coding works the same way — certain services are considered part of a larger procedure and cannot be billed separately.
The National Correct Coding Initiative (NCCI) was developed by CMS — the Centers for Medicare and Medicaid Services — to promote correct coding and prevent improper payments. NCCI edits are pairs of CPT codes that should not be billed together because one is considered a component of the other.
There are two types of NCCI edits:
| Bundled Into | Because |
|---|---|
| Surgical approach (incision and closure) | Always included in any surgical procedure code |
| Local anesthesia | Included in the surgical code — cannot bill separately |
| Simple wound closure after excision | Included in excision codes — only complex closure is separate |
| Diagnostic endoscopy with surgical endoscopy | Diagnostic scope is bundled when a therapeutic procedure is performed |
| Catheter insertion with certain procedures | Considered part of surgical approach for some procedures |
| Venipuncture with lab draw | The draw is part of the lab collection |
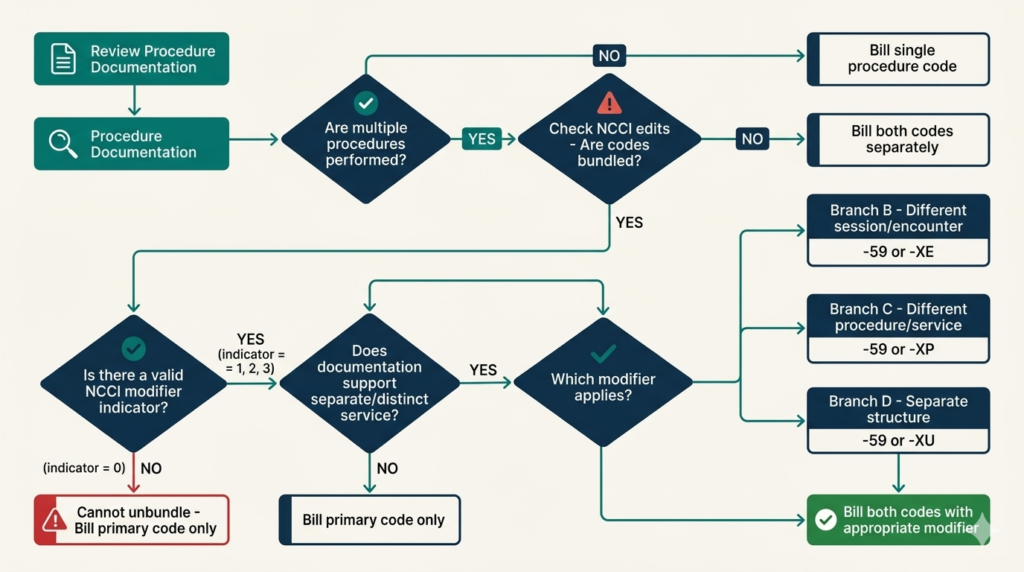
Sometimes two procedures that are normally bundled are legitimately performed as distinct, separate services on the same day. In these cases, modifier -59 (Distinct Procedural Service) can be appended to the component code to signal to the payer that the services were truly separate and both should be paid.
Modifier -59 is appropriate when the procedures were performed at a different anatomical site, during a different patient encounter, or involved a different lesion or organ. However, it must be supported by documentation — simply adding -59 without clinical justification is considered improper billing.
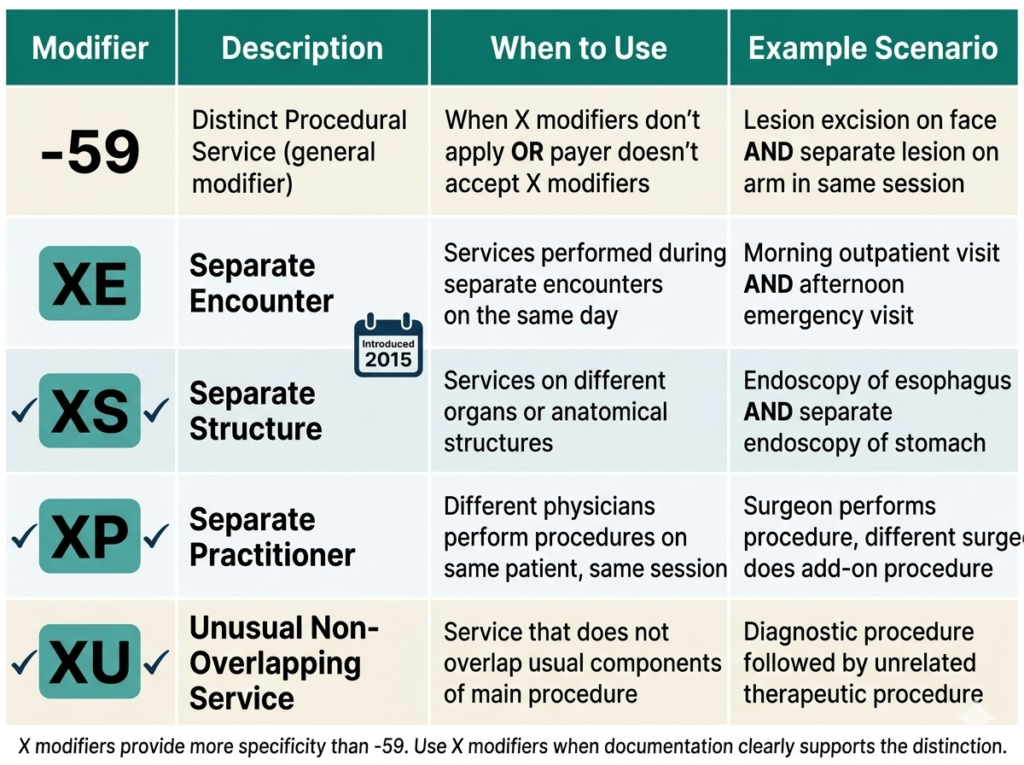
CMS created four more specific modifiers to replace modifier -59 in certain situations. These are called the X modifiers or NCCI derivative modifiers:
One of the most commonly tested bundling rules on the CPC exam involves endoscopy procedures. The rule states: when a surgical endoscopy is performed, the diagnostic endoscopy is always bundled into the surgical endoscopy code and cannot be billed separately.
For example, if a physician performs a colonoscopy and finds and removes a polyp, you code only the colonoscopy with polypectomy. You do not also code a diagnostic colonoscopy — the diagnostic scope was part of getting to the polyp and is bundled into the therapeutic code.
NCCI also includes mutually exclusive edits — pairs of codes that by definition or medical impossibility cannot reasonably be performed on the same patient on the same day. Unlike procedure-to-procedure edits where one code is a component of another, mutually exclusive codes are simply services that cannot logically both occur. For example, codes for a total and a partial removal of the same organ are mutually exclusive.
CPT modifiers are two-digit codes appended to CPT codes to provide additional information about a service without changing its definition. They tell the payer that something about the service was different from the standard — maybe it was performed on both sides of the body, or a separate service was provided on the same day, or only part of a procedure was completed. Mastering modifiers is essential for the CPC exam and for accurate real-world coding.
Without modifiers, a single CPT code describes a procedure in its most typical form. But medicine is rarely that simple. A surgeon might perform two unrelated procedures on the same day. A radiologist might only read an image without performing the technical portion. A procedure might be stopped halfway through due to a patient’s condition. Modifiers give coders the tools to accurately describe these variations without creating entirely new codes for every possible scenario.
| Modifier | Name | When to Use |
|---|---|---|
| -22 | Increased Procedural Services | Procedure required substantially more work than usual. Must have documentation supporting the increased effort. |
| -24 | Unrelated E&M During Post-op Period | E&M visit during global period for a condition unrelated to the surgery. |
| -25 | Significant Separately Identifiable E&M | E&M on same day as a minor procedure (0 or 10-day global). The E&M must be above and beyond the procedure. |
| -26 | Professional Component | Physician provided only the interpretation and report of a radiology or other diagnostic service. |
| -32 | Mandated Services | Service was required by a payer, governmental, or regulatory entity. |
| -47 | Anesthesia by Surgeon | Regional or general anesthesia was provided by the operating surgeon (rare). |
| -50 | Bilateral Procedure | Procedure performed on both sides of the body during the same session. |
| -51 | Multiple Procedures | Multiple procedures performed at same session by same provider. Primary procedure listed first, others with -51. |
| -52 | Reduced Services | Procedure was partially reduced at physician’s discretion. Less than the full service was performed. |
| -53 | Discontinued Procedure | Procedure started but stopped due to patient’s condition. Different from -52 which is elective reduction. |
| -54 | Surgical Care Only | One physician performed the surgery; another will provide pre- and post-op care. |
| -55 | Postoperative Management Only | Physician provided only post-op care; another performed the surgery. |
| -56 | Preoperative Management Only | Physician provided only pre-op care; another performed the surgery. |
| -57 | Decision for Surgery | E&M visit resulted in initial decision to perform major surgery (90-day global). Appended to the E&M code. |
| -58 | Staged/Related Procedure During Post-op | Planned follow-up procedure during the global period, or procedure more extensive than anticipated. |
| -59 | Distinct Procedural Service | Procedure is distinct from another on the same day — different session, site, lesion, or organ system. |
| -62 | Two Surgeons | Two surgeons each performing distinct parts of a procedure. Each bills with -62. |
| -63 | Procedure on Infant | Procedure performed on infant weighing less than 4 kg. |
| -66 | Surgical Team | Complex procedure requiring a team of surgeons of different specialties simultaneously. |
| -76 | Repeat Procedure by Same Physician | Procedure repeated by the same physician on the same day. |
| -77 | Repeat Procedure by Different Physician | Procedure repeated by a different physician on the same day. |
| -78 | Return to OR for Related Complication | Unplanned return to operating room for a complication related to the original surgery. |
| -79 | Unrelated Procedure During Post-op Period | New, unrelated procedure performed during the global period of a previous surgery. |
| -80 | Assistant Surgeon | Physician assisted the primary surgeon. Bills at a percentage of the primary surgeon’s fee. |
| -TC | Technical Component | Only the technical portion of a service was provided (equipment, staff, facility — not interpretation). |
These two modifiers both involve an E&M service alongside a procedure, but they apply in different situations:
All three involve procedures during a post-operative global period, but for different reasons:
In addition to CPT modifiers (two digits), coders also use HCPCS Level II modifiers (two letters or a letter and number). Examples include:
Endoscopy coding appears on the CPC exam in multiple sections — digestive, respiratory, and urinary system procedures all involve scope-based techniques. The good news is that once you understand the core bundling rule and how endoscopy code ranges are organized, the coding logic is consistent across all body systems. This guide teaches you the fundamental rules and applies them to the most commonly tested procedures.
An endoscopy is a procedure in which a flexible or rigid scope — a tube with a camera and light — is inserted into the body to visualize internal structures. Depending on the body area, endoscopes are introduced through natural openings such as the mouth, anus, or urethra, or through small surgical incisions. Endoscopy can be purely diagnostic or can involve therapeutic interventions such as biopsy, polyp removal, or foreign body extraction.
This is the single most tested endoscopy concept on the CPC exam. The rule states:
For example, if a physician performs a colonoscopy and removes a polyp, you code only the colonoscopy with polypectomy. You do not also code a diagnostic colonoscopy. The diagnostic scope was the approach to the polyp removal and is bundled into the therapeutic code.
However, if a physician performs a diagnostic colonoscopy and finds nothing requiring treatment, you code the diagnostic colonoscopy alone — there is no therapeutic code to bundle it into.
Colonoscopy is examined on nearly every CPC exam. The codes are organized by what was done during the procedure:
| CPT Code | Description |
|---|---|
| 45378 | Colonoscopy, diagnostic, with or without collection of specimen(s) by brushing or washing |
| 45380 | Colonoscopy with biopsy, single or multiple |
| 45381 | Colonoscopy with directed submucosal injection |
| 45382 | Colonoscopy with control of bleeding |
| 45384 | Colonoscopy with removal of tumor, polyp, or lesion by hot biopsy forceps |
| 45385 | Colonoscopy with removal of tumor, polyp, or lesion by snare technique |
| 45386 | Colonoscopy with dilation of stricture |
EGD involves passing a scope through the mouth into the esophagus, stomach, and duodenum. The code range is 43235–43259. Similar to colonoscopy, codes are selected based on what therapeutic intervention was performed:
Bronchoscopy involves passing a scope into the airways — the trachea and bronchi. The code range is 31622–31651. Key codes include:
Cystoscopy involves passing a scope through the urethra into the bladder. The code range is 52000–52355:
Sometimes an endoscopy is started but cannot be completed due to the patient’s condition or an unexpected finding. In this case, modifier -53 (Discontinued Procedure) is appended to indicate that the procedure was started but not completed. This is different from modifier -52 (Reduced Services), which is used when the physician electively performs less than the full service.
Evaluation and Management codes — commonly called E&M codes — are the most frequently used codes in all of outpatient medical billing. Every office visit, every hospital encounter, every consultation involves an E&M code. For the CPC exam, E&M coding is tested heavily and the 2023 revised guidelines changed how these codes are selected. This guide covers everything a beginner needs to understand E&M coding from the ground up.
E&M codes describe physician or qualified healthcare professional visits and services — the face-to-face (or now telehealth) encounters where a patient is evaluated and managed. They cover office visits, hospital admissions, emergency department encounters, nursing facility visits, home visits, and more. E&M codes are found in the 99202–99499 range of the CPT codebook.
Unlike surgery codes that describe a specific procedure, E&M codes capture cognitive work — the thinking, evaluating, and decision-making that physicians do when they assess and treat patients.
The first determination in outpatient E&M coding is whether the patient is new or established to the practice. This matters because new patient visits have different code numbers and generally higher reimbursement than established patient visits.
| Patient Type | Code Range | Levels |
|---|---|---|
| New patient — office or outpatient | 99202–99205 | 4 levels (level 1 deleted in 2021) |
| Established patient — office or outpatient | 99211–99215 | 5 levels |
Note that 99211 (established patient, minimal service) does not require physician presence — it is used for services performed by clinical staff under physician supervision, such as a nurse taking a blood pressure reading.
Before 2021, E&M level selection was based on three components — history, physical examination, and medical decision making. The 2021 and 2023 guidelines eliminated the documentation-counting approach for office visits and replaced it with two options: Medical Decision Making (MDM) or Total Time.
MDM is based on three elements. The overall MDM level is determined by meeting or exceeding requirements in at least two of the three elements:
| MDM Level | Code (New) | Code (Est.) | Problems | Data | Risk |
|---|---|---|---|---|---|
| Straightforward | 99202 | 99212 | Minimal | Minimal/none | Minimal |
| Low complexity | 99203 | 99213 | Low | Limited | Low |
| Moderate complexity | 99204 | 99214 | Moderate | Moderate | Moderate |
| High complexity | 99205 | 99215 | High | Extensive | High |
Physicians may also select the E&M level based on total time spent on the date of the encounter — including not just face-to-face time but also time spent reviewing records, ordering tests, coordinating care, and documenting. The time ranges for each level are specified in the CPT guidelines and vary between new and established patients.
Beyond office visits, several other E&M categories are frequently tested:
The global surgical package is one of the most heavily tested concepts on the CPC exam — and one of the most misunderstood by beginner coders. Understanding it thoroughly is essential not just for the exam, but for accurate real-world coding. This article breaks it down completely, from what the global package includes to how modifiers are used to break it apart when necessary.
When a surgeon performs a procedure and bills a CPT surgical code, that code does not just cover the operation itself. It covers a bundle of related services provided before, during, and after the surgery — all included in a single payment. This bundle is called the global surgical package.
The concept was created by Medicare and adopted widely across payers to simplify payment for surgical care. Instead of billing separately for every pre-operative visit, the surgery, and every post-operative follow-up, the surgeon receives one global payment that covers all of it within the global period.
The following services are bundled into the global surgical fee and cannot be billed separately:
Certain services can still be billed separately even during the global period:
Not all surgical procedures have the same global period. Medicare assigns each surgical code one of three global period designations:
| Global Period | What It Means | Examples |
|---|---|---|
| 0-Day Global | No post-operative period. The surgical package only covers the procedure itself and same-day care. | Minor procedures like shave removals, needle biopsies |
| 10-Day Global | Post-operative period lasts 10 days after the procedure date. Related follow-up visits within 10 days are included. | Excision of skin lesions, simple repairs |
| 90-Day Global | Post-operative period lasts 90 days. Also includes one pre-operative day. Major surgical procedures fall here. | Appendectomy, CABG, total knee replacement, hysterectomy |
Modifiers are used to signal to payers that a service should be paid separately despite the global period rules. These are among the most tested modifiers on the CPC exam:
| Modifier | When to Use It |
|---|---|
| -24 | Unrelated E&M service during a post-operative period. The visit is for a completely different condition than the surgery. |
| -25 | Significant, separately identifiable E&M service on the same day as a minor procedure (0 or 10-day global). The E&M must be above and beyond what is included in the procedure. |
| -57 | Decision for surgery. The E&M visit resulted in the initial decision to perform a major (90-day global) surgery. Appended to the E&M code, not the surgery code. |
| -58 | Staged or related procedure during the post-operative period. The follow-up procedure was planned or is more extensive than expected. |
| -78 | Unplanned return to the OR for a related complication during the post-operative period. |
| -79 | Unrelated procedure during the post-operative period. The new surgery is for a completely different condition. |
Here is a scenario that illustrates global package rules in action:
A patient sees Dr. Smith on Monday for abdominal pain. After evaluation, Dr. Smith decides the patient needs an appendectomy (a 90-day global procedure). Surgery is performed on Wednesday. The patient returns two weeks later with a wound infection that Dr. Smith treats in the office. Four weeks later, the patient comes in for a completely unrelated sinus infection.
One of the first things every beginner coder needs to understand is how the CPT codebook is physically organized. Knowing where to look — and how codes are numbered — saves you enormous time, both in daily coding work and on the CPC exam where every minute counts. This article walks you through the complete structure of the CPT codebook from the inside out.
Not all CPT codes work the same way. The AMA divides CPT codes into three distinct categories, each serving a different purpose:
Category I codes are the five-digit numeric codes you will use for the vast majority of your coding work. These codes describe procedures and services that are widely performed, have proven clinical efficacy, and are approved by the FDA where applicable. The CPT codebook is organized into six sections of Category I codes:
| Section | Code Range | What It Covers |
|---|---|---|
| Evaluation & Management | 99202–99499 | Office visits, hospital care, consults, preventive medicine |
| Anesthesia | 00100–01999 | Anesthesia services for surgical procedures |
| Surgery | 10004–69990 | All surgical procedures by body system |
| Radiology | 70010–79999 | Imaging, radiation oncology, nuclear medicine |
| Pathology & Laboratory | 80047–89398 | Lab tests, cultures, surgical pathology |
| Medicine | 90281–99607 | Vaccines, infusions, ophthalmology, psychiatry |
Category II codes are four-digit codes followed by the letter F (for example, 0001F). These are supplemental tracking codes used for performance measurement — they help track whether providers are following clinical guidelines, such as documenting blood pressure for hypertensive patients. Category II codes are optional and are never used as a substitute for Category I codes. They are not tested heavily on the CPC exam but you should know what they are.
Category III codes are four-digit codes followed by the letter T (for example, 0042T). These are temporary codes for new, experimental, or emerging technologies and procedures that do not yet qualify for Category I status. If a Category III code exists for a procedure, it must be used instead of an unlisted code. After five years, a Category III code is either promoted to Category I or deleted.
Since surgery makes up approximately 40% of the CPC exam, understanding how that section is structured is especially important. The Surgery section is divided into subsections by body system:
At the back of the CPT codebook is an alphabetic index — your starting point for finding any code. The index lists procedures, services, organs, conditions, and eponyms. However, a critical rule that every coder must follow is this: never code directly from the index. The index points you to a code range; you must always verify the final code in the main section of the codebook.
The index has four types of main entries:
At the beginning of each CPT section — and sometimes before subsections — you will find guidelines. These are essential instructions that explain how codes in that section should be used, what is included and excluded, and how to apply modifiers. Reading guidelines carefully is non-negotiable for accurate coding.
For example, the Surgery section guidelines explain the global surgical package — what is included in a surgical code before, during, and after a procedure. The E&M guidelines explain how to determine the level of service. On the CPC exam, many questions are designed specifically to test whether you have read and understood these guidelines.
The CPT codebook includes several appendices that contain important reference information:
Tab Appendix A in your exam book — the modifier list is referenced frequently during the CPC exam and having it marked saves valuable time.
The CPT codebook uses symbols throughout to give coders additional information at a glance. Learn these before your exam:
| Symbol | Meaning |
|---|---|
| ● (Bullet) | New code added in this edition |
| ▲ (Triangle) | Code description has been revised |
| + (Plus) | Add-on code — never reported alone |
| ⊘ (Circle with slash) | Modifier -51 exempt |
| ★ (Star) | Telemedicine service |
| # (Hash) | Code is out of numerical sequence |
The CPT Alphabetic Index is found at the back of the CPT codebook and is your starting point for finding any procedure code. Used correctly it saves you enormous time during coding and on the CPC exam. Used incorrectly it can send you to the wrong section entirely. This guide teaches you exactly how the index works and the strategies experienced coders use to find codes quickly and accurately.
Before anything else, memorize this rule and never break it:
The index points you in the right direction but it does not tell you everything. The main section contains guidelines, notes, parenthetical instructions, and full descriptions that are essential for accurate code selection. The index is a navigation tool — not the destination.
The CPT index is organized alphabetically by main entries. There are four types of main entries and knowing all four gives you multiple routes to find any code:
The most common starting point. Look up what was done. Examples: Appendectomy, Biopsy, Debridement, Excision, Repair, Replacement. This works well when the operative report clearly states the procedure name.
Look up the body part involved. Examples: Appendix, Knee, Lung, Stomach. Under each anatomic site you will find subentries organized by what was done to that structure. This is useful when you know where the procedure was performed but are unsure of the exact procedure name.
Look up the diagnosis or condition being treated. Examples: Fracture, Hernia, Infection, Tumor. Subentries then break down by treatment type or anatomic location. This approach works well when you start with the diagnosis rather than the procedure name.
Some procedures are known by the name of the surgeon who developed them. Examples: Whipple Procedure (pancreaticoduodenectomy), Nissen Fundoplication, Colles Fracture repair. If you see an unusual procedure name in an operative report, try looking it up as an eponym in the index.
Main entries in the index are followed by indented subterms that narrow down the search. Subterms may describe the anatomic site, the approach, the method, or the indication. Reading subterms carefully is essential — the wrong subterm leads to the wrong code range.
For example, under the main entry “Excision” you will find dozens of subterms: Lesion, Tumor, Cyst, each broken down further by anatomic location. Under “Lesion” you will find subterms like Skin, Soft Tissue, Bone — and under each of those, further subterms for benign vs malignant or location-specific breakdowns.
The index may point you to different types of references:
During the CPC exam you have approximately 2 minutes and 15 seconds per question. Index navigation speed directly affects your score. Here are strategies experienced coders use:
Skin lesion excision coding is one of the most calculation-intensive topics on the CPC exam. Every question requires you to correctly classify the lesion, measure it with margins, locate the right code range, and decide whether a separate repair code applies. Once you learn the systematic approach, these questions become some of the most predictable and manageable on the entire exam.
CPT divides skin lesion excisions into two categories based on the nature of the lesion:
Within each category, codes are further organized by anatomical location and excised diameter in centimeters. Malignant lesion codes generally reimburse at a higher rate than benign codes because the excision technique and margins required are more extensive.
This is the rule that most beginners miss. When coding a lesion excision, you do not use the size of the lesion alone. You use the size of the lesion plus the margins taken around it.
The correct measurement formula is:
Why multiply the margin by 2? Because margins are taken on all sides of the lesion. A 0.5 cm margin around a circular lesion adds 0.5 cm on one side and 0.5 cm on the other — totaling 1.0 cm added to the lesion diameter.
A physician excises a benign lesion on the back. The lesion measures 1.2 cm and 0.3 cm margins are taken.
| Location | Code Range |
|---|---|
| Trunk, arms, or legs | 11400–11406 |
| Scalp, neck, hands, feet, or genitalia | 11420–11426 |
| Face, ears, eyelids, nose, lips, or mucous membranes | 11440–11446 |
| Location | Code Range |
|---|---|
| Trunk, arms, or legs | 11600–11606 |
| Scalp, neck, hands, feet, or genitalia | 11620–11626 |
| Face, ears, eyelids, nose, lips, or mucous membranes | 11640–11646 |
After a lesion excision, the wound must be closed. Whether you can bill a separate repair code depends on the complexity of the closure:
When multiple lesions are excised during the same encounter, each lesion is coded separately. Unlike wound repairs, lesion excision lengths are NOT added together. Each lesion gets its own CPT code based on its own excised diameter and location. Report additional lesions with modifier -59 if needed to bypass NCCI edits.