Table of Contents
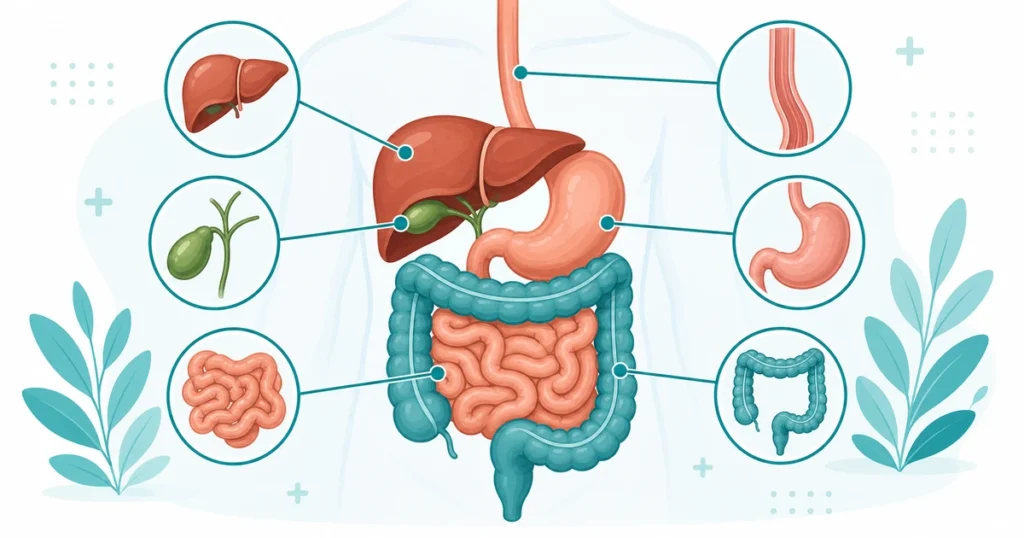
The digestive system — also called the gastrointestinal (GI) tract — is responsible for breaking down food, absorbing nutrients, and eliminating waste. As a medical coder, you will encounter digestive system conditions constantly, from simple gastroenteritis to complex surgical cases involving multiple organs. Understanding digestive anatomy and terminology ensures you code these conditions accurately, and it forms the foundation for the Digestive System CPT coding section (40490–49999) on the CPC exam.
This guide covers the entire GI tract from mouth to anus, the accessory organs of digestion, essential digestive terminology with root words and suffixes, high-yield endoscopy and surgical codes, and the coding rules the CPC exam tests most often.
The GI Tract — From Mouth to Anus
The digestive system is essentially one continuous tube from the mouth to the anus, with several specialized regions. Each region has specific functions, associated conditions, and its own CPT code ranges. Knowing the anatomical order is a prerequisite for the CPC exam.
Mouth (Oral Cavity)
Digestion begins in the mouth. Mechanical digestion occurs through chewing (mastication), while chemical digestion starts with salivary enzymes — specifically amylase, which breaks down starches. Key structures include the tongue, teeth, salivary glands (parotid, submandibular, sublingual), hard palate, and soft palate.
Common conditions include stomatitis (mouth inflammation), gingivitis (gum inflammation), dental caries, oral leukoplakia, oral thrush (candidiasis), and cleft palate.
Oral cavity procedures may be coded from the Digestive System CPT section (40000–40899) or from the Dental section. The floor of the mouth, vestibule, tongue, and lips each have separate code ranges — always identify the exact oral structure from the operative report.
Pharynx and Esophagus
The pharynx (throat) connects the mouth to the esophagus and also serves the respiratory system. The esophagus is a muscular tube approximately 25 cm long that transports food from the pharynx to the stomach through peristalsis — rhythmic muscle contractions that push food downward.
Two sphincters control the esophagus. The upper esophageal sphincter (UES) prevents air from entering the esophagus during breathing. The lower esophageal sphincter (LES) prevents stomach acid from refluxing back into the esophagus. Dysfunction of the LES causes GERD (gastroesophageal reflux disease), one of the most commonly coded GI diagnoses.
| Condition | What It Is | Coding Note |
|---|---|---|
| GERD (K21.-) | Chronic acid reflux from LES dysfunction | K21.0 with esophagitis, K21.9 without |
| Barrett’s esophagus (K22.7-) | Precancerous change from chronic GERD | Specify with or without dysplasia |
| Esophageal stricture (K22.2) | Narrowing of the esophagus | Often treated with dilation (43450–43453) |
| Esophageal varices (I85.-) | Enlarged veins from portal hypertension | Specify with or without bleeding |
| Dysphagia (R13.-) | Difficulty swallowing | Specify oral, oropharyngeal, or other phase |
| Achalasia (K22.0) | Failure of the LES to relax | May require Heller myotomy (43279) |
Esophageal procedures include EGD (esophagogastroduodenoscopy), dilation, stenting, and fundoplication (surgical repair for GERD). The endoscopy procedure coding guide covers the rules for coding these procedures, including the critical bundling rules.
Stomach
The stomach is a J-shaped organ that stores food, mixes it with gastric juices containing hydrochloric acid and pepsin, and begins protein digestion. It has four anatomical regions: the cardia (where the esophagus connects), the fundus (upper dome), the body (main portion), and the antrum/pylorus (lower portion connecting to the duodenum).
The pyloric sphincter controls the release of partially digested food (chyme) into the duodenum. The rugae are folds in the stomach lining that allow the stomach to expand when filled.
Common conditions include gastritis, peptic ulcer disease (both gastric and duodenal ulcers), gastric cancer, gastroparesis (delayed stomach emptying), and hiatal hernia. For coding peptic ulcers, ICD-10-CM requires specificity about the site (gastric vs. duodenal), whether it is acute or chronic, and whether there is hemorrhage or perforation — a four-axis classification that produces many possible code combinations.
Gastric procedures include gastrectomy (partial or total), gastric bypass, vagotomy, pyloroplasty, and endoscopic procedures such as biopsy, foreign body removal, and hemostasis. Bariatric surgery codes (43770 series) are increasingly tested on the CPC exam.
Small Intestine
The small intestine is approximately 20 feet long and is the primary site of nutrient absorption. It has three sections, each with distinct functions:
The duodenum is the first and shortest section at about 10 inches. It receives bile from the gallbladder and digestive enzymes from the pancreas via the ampulla of Vater. Most chemical digestion occurs here. The jejunum is the middle section at about 8 feet and is the primary site of carbohydrate and protein absorption. It has a thicker wall and more villi — finger-like projections that increase surface area — than the ileum. The ileum is the final and longest section at about 12 feet. It absorbs vitamin B12 and bile salts and connects to the large intestine at the ileocecal valve.
Small intestine procedure codes are in the 44005–44799 range. Important procedures include enterotomy, resection with anastomosis, and Meckel’s diverticulectomy. Endoscopic procedures of the small intestine use enteroscopy codes.
Large Intestine (Colon)
The large intestine is approximately 5 feet long and is responsible for water reabsorption and stool formation. It consists of several distinct sections that coders must know by name and position.
| Section | Location | Clinical Significance |
|---|---|---|
| Cecum | Beginning, connected to ileum | Appendix attaches here |
| Ascending colon | Right side, runs upward | Right hemicolectomy territory |
| Hepatic flexure | Bend near the liver | Transition from ascending to transverse |
| Transverse colon | Crosses horizontally | Longest and most mobile segment |
| Splenic flexure | Bend near the spleen | Transition from transverse to descending |
| Descending colon | Left side, runs downward | Left hemicolectomy territory |
| Sigmoid colon | S-shaped, connects to rectum | Most common site of diverticulosis |
Common conditions include ulcerative colitis, diverticulitis and diverticulosis, colorectal cancer, colonic polyps, irritable bowel syndrome (IBS), volvulus (twisting), and intussusception.
Colonoscopy codes (45378 series) are among the most commonly tested digestive system codes on the CPC exam. Surgical colectomy codes (44140–44160) are organized by the extent of resection — segmental, hemicolectomy, or total.
Rectum and Anus
The rectum stores stool before elimination. The anus is the external opening controlled by internal (involuntary) and external (voluntary) sphincter muscles.
Common conditions include hemorrhoids (internal and external), anal fissures, rectal prolapse, rectal cancer, perianal abscess, and anal fistula. Hemorrhoid procedures (46200–46262) are commonly tested — know the difference between internal and external hemorrhoids and the various treatment methods including banding, excision, ligation, and stapled hemorrhoidopexy.
Accessory Organs of Digestion
Several organs support digestion without being part of the main GI tract. These accessory organs produce enzymes, bile, and hormones essential for breaking down food.
Liver
The liver is the largest internal organ, located in the right upper quadrant of the abdomen. It produces bile to digest fats, metabolizes nutrients, filters blood, stores glycogen, produces clotting factors, and detoxifies harmful substances.
The liver has two main lobes (right and left) and is connected to the gallbladder via the common hepatic duct. The hepatic portal vein brings nutrient-rich blood from the intestines to the liver for processing.
Common conditions include hepatitis (A, B, C — viral inflammation), cirrhosis (scarring from chronic liver damage), fatty liver disease (NAFLD/NASH), hepatocellular carcinoma, and portal hypertension. For hepatitis coding, ICD-10-CM distinguishes between acute and chronic forms, the specific virus type, and the presence or absence of hepatic coma — each axis adds specificity to the code. This is similar to the multi-axis classification used in diabetes coding.
Liver procedures include hepatectomy (partial liver resection), liver biopsy, ablation of liver tumors, and TIPS procedure (transjugular intrahepatic portosystemic shunt for portal hypertension).
Pancreas
The pancreas is located behind the stomach in the retroperitoneal space and has both exocrine (digestive enzyme production) and endocrine (hormone production — insulin and glucagon) functions.
The head of the pancreas is cradled by the duodenum. The pancreatic duct joins the common bile duct at the ampulla of Vater (hepatopancreatic ampulla), which opens into the duodenum. The sphincter of Oddi controls the flow of bile and pancreatic juice into the duodenum.
Common conditions include acute pancreatitis (often caused by gallstones or alcohol), chronic pancreatitis, pancreatic cancer (frequently in the head of the pancreas), and pancreatic cysts.
ERCP (endoscopic retrograde cholangiopancreatography) codes (43260–43278) are also commonly tested. ERCP is both a diagnostic and therapeutic procedure — know that diagnostic ERCP is bundled into therapeutic ERCP, following the standard endoscopy bundling rule.
Gallbladder and Biliary System
The gallbladder stores and concentrates bile produced by the liver. During fat digestion, the gallbladder contracts and releases bile through the cystic duct into the common bile duct, then into the duodenum.
The biliary system includes the right and left hepatic ducts, common hepatic duct, cystic duct, and common bile duct (CBD). The CBD joins the pancreatic duct at the ampulla of Vater.
| Condition | Root/Term | Meaning |
|---|---|---|
| Cholelithiasis | chol/e (bile) + lith (stone) + -iasis | Gallstones |
| Cholecystitis | cholecyst/o (gallbladder) + -itis | Gallbladder inflammation |
| Choledocholithiasis | choledoch/o (common bile duct) + lith + -iasis | Stones in the common bile duct |
| Cholangitis | cholangi/o (bile duct) + -itis | Bile duct infection |
| Biliary dyskinesia | dys- (abnormal) + kinesi (movement) | Abnormal gallbladder contraction |
Cholecystectomy (gallbladder removal) is one of the most commonly performed surgeries. Know the difference between laparoscopic cholecystectomy (47562–47564) and open cholecystectomy (47600–47620), and know cholangiography codes for imaging the bile ducts during surgery.
Essential Digestive Terminology
Root Words (Combining Forms)
The digestive system has the most root words of any body system. The highest-yield roots are: or/o and stomat/o (mouth), esophag/o (esophagus), gastr/o (stomach), enter/o (small intestine), duoden/o (duodenum), jejun/o (jejunum), ile/o (ileum), col/o and colon/o (colon), sigmoid/o (sigmoid colon), rect/o and proct/o (rectum), an/o (anus), hepat/o (liver), cholecyst/o (gallbladder), choledoch/o (common bile duct), pancreat/o (pancreas), and chol/e (bile/gall).
Surgical vs. Diagnostic Suffixes
Surgical suffixes you will see in operative reports: -ectomy (removal), -otomy (incision into), -ostomy (creating an opening), -plasty (repair), -scopy (scope examination), -pexy (fixation), -rraphy (suturing), and -stasis (stopping/controlling — as in hemostasis).
Diagnostic suffixes that appear in clinical notes: -itis (inflammation), -osis (abnormal condition), -emesis (vomiting — hematemesis is vomiting blood), -phagia (swallowing — dysphagia is difficulty swallowing), and -pepsia (digestion — dyspepsia is indigestion).
Key Endoscopy Codes for the CPC Exam
Endoscopic procedures of the digestive system are the most commonly tested GI codes. Here are the highest-yield codes:
| CPT Code | Procedure | Key Detail |
|---|---|---|
| 43235 | EGD, diagnostic | Visualizes esophagus, stomach, duodenum |
| 43239 | EGD with biopsy | Includes diagnostic EGD — do not report 43235 separately |
| 43247 | EGD with foreign body removal | Includes diagnostic — bundling rule applies |
| 43249 | EGD with balloon dilation | Common for esophageal stricture |
| 45378 | Colonoscopy, diagnostic | Rectum to cecum visualization |
| 45380 | Colonoscopy with biopsy | Includes diagnostic — do not report 45378 separately |
| 45385 | Colonoscopy with snare polypectomy | Snare technique for polyp removal |
| 45388 | Colonoscopy with ablation | Lesion ablation during colonoscopy |
CPC Exam Tips for Digestive System Coding
The CPC exam tests digestive system coding more heavily than most other body systems. The six highest-yield topics are: (1) the anatomical order of the GI tract — questions test whether you can identify where a condition occurs; (2) endoscopy bundling — diagnostic is always bundled into surgical; (3) laparoscopic vs. open approach — always identify the surgical approach because it determines the code; (4) biliary terminology — the chole/cholecyst/choledoch/cholangi pattern; (5) the Whipple procedure (48150) — know which structures are resected; and (6) appendectomy codes — 44950 (open) vs. 44970 (laparoscopic).
5 quick questions drawn from this guide. Click an answer to check it — explanations appear as you go.
1. The correct path of the GI tract is:
2. The accessory organs of digestion are the:
3. The three parts of the small intestine, in order, are:
4. The suffix ‘-ectomy’ means:
5. A colonoscopy examines the:
Frequently Asked Questions
What is the most commonly tested digestive system topic on the CPC exam?
Endoscopy coding — specifically colonoscopy and EGD codes with the bundling rule. If a diagnostic endoscopy and a surgical endoscopy are performed at the same session in the same area, report only the surgical code. This rule appears on nearly every CPC exam.
How do I distinguish Crohn’s disease from ulcerative colitis in coding?
Crohn’s disease (K50.-) can affect any part of the GI tract and is coded by location — small intestine, large intestine, or both. Ulcerative colitis (K51.-) affects only the colon and rectum. ICD-10-CM codes for both specify whether the condition is with or without complications such as abscess, fistula, or intestinal obstruction.
What is the difference between a colostomy and a colectomy?
A colostomy (-ostomy = creating an opening) is a procedure that brings the colon to the abdominal surface to create a stoma for waste elimination. A colectomy (-ectomy = removal) is the surgical removal of part or all of the colon. A patient may have both procedures in the same operative session — the colon is resected (colectomy) and then a stoma is created (colostomy).
Why is biliary terminology so important for the CPC exam?
The gallbladder and bile duct system uses a unique set of Greek-derived roots — chol/e (bile), cholecyst/o (gallbladder), choledoch/o (common bile duct), cholangi/o (bile duct). These roots appear in condition names (cholelithiasis, cholecystitis, choledocholithiasis, cholangitis), procedure names (cholecystectomy, choledocholithotomy, cholangiography), and imaging studies (ERCP). Memorizing this root family eliminates guessing on a significant block of CPC exam questions.
How are bariatric surgery codes tested?
Bariatric codes (43770 series) are increasingly common on the CPC exam. Key codes include 43775 (sleeve gastrectomy), 43644 (laparoscopic Roux-en-Y gastric bypass), and 43770 (laparoscopic gastric restrictive procedure — band placement). Know the anatomical difference between these procedures — a sleeve removes part of the stomach, a bypass reroutes the small intestine, and a band restricts the stomach opening.